Public health professionals are often called to do the work that they do. They are dedicated to protecting and improving the health of communities. They are often driven by passion and fueled by a desire to make a tangible difference in people's lives. But who are they?
In the U.S., the public health workforce is aligned somewhat closely to the U.S. population in terms of diversity, but a major difference is the representation of women. Women make up the majority of the U.S. public health workforce (79%). From 2005 to 2016, 70-73% of all public health degrees in the U.S. were awarded to women.
Looking globally, women make up 69% of the global health and social care workforce. Women provide essential health services for an estimated 5 billion people worldwide, making our input into global health systems over US$3 trillion annually.
However, a paradox emerges when we look at leadership positions within public health. While women make up the backbone of the public health workforce, men disproportionately hold leadership roles, from directors of public health agencies to CEOs of major health organizations. These disparities are more pronounced among women with intersectional identities (e.g., women of color). 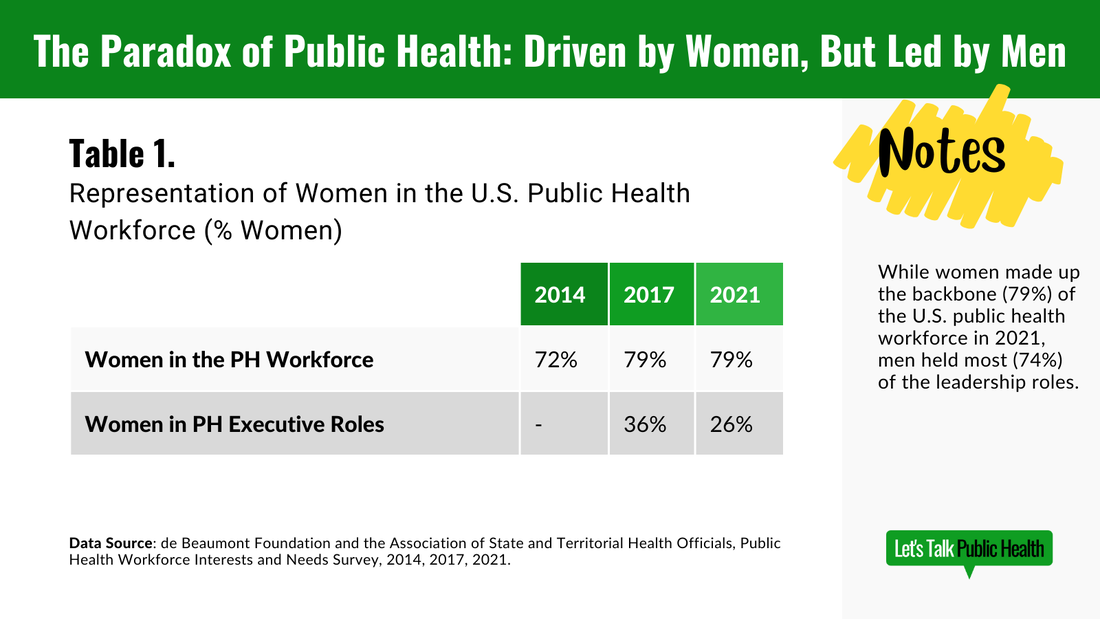
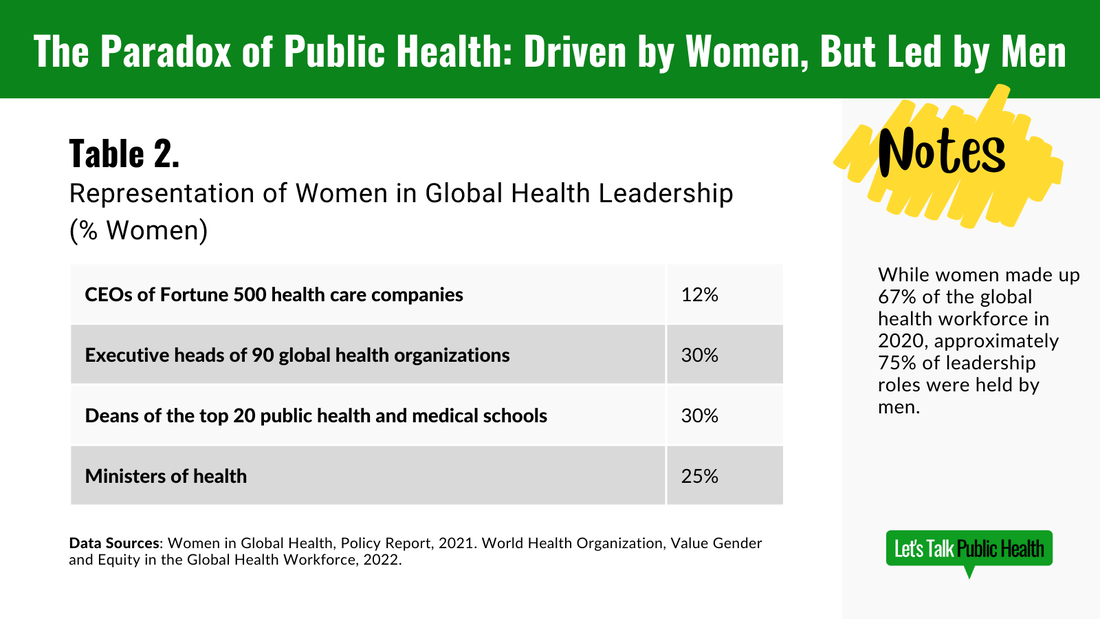
Women health workers tend to be employed in roles given lower social value, status, and pay, like public health nursing and unpaid community health work. Men are the majority of surgeons, policymakers, and high-paying leadership roles. Approximately 75% of leadership roles in global health are held by men.
Not only are men overrepresented in leadership, but they’re also making more money than their female counterparts. In 2014, women in the U.S. public health workforce earned $6,000 less per year than men, and were less likely to hold an executive leadership position. In 2017, women in leadership roles in women in the U.S. public health workforce earned about $3,000 less per year than their male counterparts, and that gap increased at the executive level. By 2018, the pay gap for female employees in the U.S. Department of Health and Human Services decreased from earning about 13% less than men in 2010 to 9.2% less. Globally, in 2022, women in the health and care workforce earned 15-24% less than their male counterparts. This creates a crucial question that we should be asking ourselves, especially during Women’s History Month: Why is there such a stark discrepancy between the composition of the workforce and its leadership?
Several systemic factors contribute to this gender gap:
Addressing this disparity requires a multifaceted approach that needs to start now.
We cannot wait the 140 years it is estimated to take for women to achieve equal leadership positions. Women in the public health and healthcare workforce are burnt out and planning to leave, and the world can’t afford to lose them. The U.S. public health workforce is already facing a shortage of 80,000 workers, and the global health workforce is facing a shortage of 10 million workers.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
�
Learn about our blog submission guidelines. >>
The views and opinions expressed by individual authors on this blog are their own and do not necessarily reflect the official policy or position of Let's Talk Public Health.
Categories
All
|
 RSS Feed
RSS Feed